{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}













{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}








{kind=link}
{kind=link}
{kind=link}










 A pain pump is essentially a balloon filled with local anesthetic that drizzles the anesthetic under the skin via small tubes placed internally at the time of surgery. The tubes are removed 3-5 days after surgery. I have never liked pain pumps and no longer use them. Exparel, discussed below, while more expensive, works much better.
A pain pump is essentially a balloon filled with local anesthetic that drizzles the anesthetic under the skin via small tubes placed internally at the time of surgery. The tubes are removed 3-5 days after surgery. I have never liked pain pumps and no longer use them. Exparel, discussed below, while more expensive, works much better.
 Exparel is a medication used to manage post-surgical pain. While not new, it is a “newer” drug that is still under patent. That it is why it is so expensive – there is no generic yet. It combines a long acting local anesthetic in a slow release formula that lasts as long as 4 days. It is injected, while the patient is asleep, into the abdominal nerves and give a “pain block.” Patients require less medication and are far more comfortable early on. I feel is does much better than pain pumps and I strongly recommend it.
Exparel is a medication used to manage post-surgical pain. While not new, it is a “newer” drug that is still under patent. That it is why it is so expensive – there is no generic yet. It combines a long acting local anesthetic in a slow release formula that lasts as long as 4 days. It is injected, while the patient is asleep, into the abdominal nerves and give a “pain block.” Patients require less medication and are far more comfortable early on. I feel is does much better than pain pumps and I strongly recommend it.
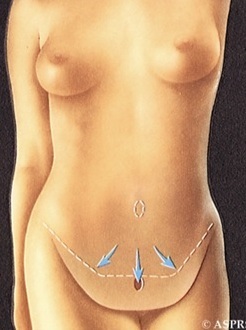
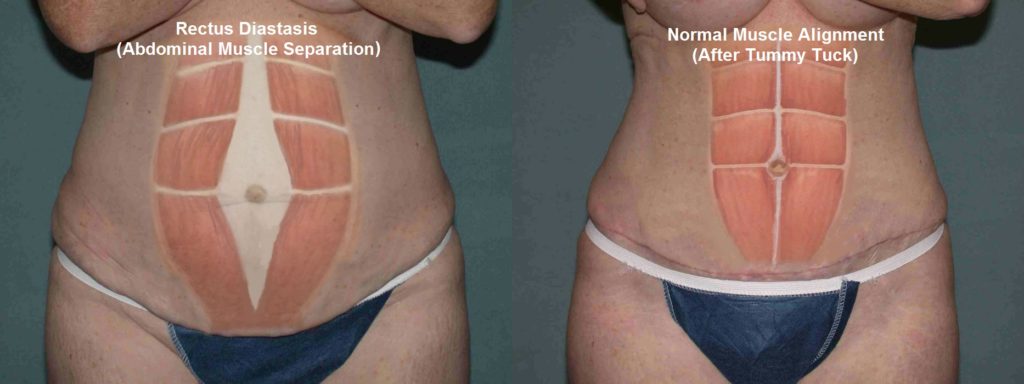
When a tummy is tightened with muscle repair the pressure inside the abdomen goes up. This can slow blood flow coming back from the legs and, in some cases, lead to blood clots. In rare cases, blood clots can break off, go to the lungs and cause death. All plastic surgeons take measures to diminish this risk. All patients in my practice get leg compression stockings and have compression balloons placed on the legs to promote blood flow and diminish clot risk. Each patient gets a small dose of a blood thinner as well. It is a fine line because we don’t want blood clots, but we don’t want bleeding either.
Some patients will purchase home compression stockings as well (seen below). These can be bought on Amazon
Most importantly, walking at home and moving the legs helps decrease the clot risk.

{kind=link}
{kind=link}
{kind=link}
{kind=link}


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
![]() The son of artist and a clergyman, Dr. Adam Tattelbaum grew up in a household where artistry and enhancing the lives of others took equal place. “I always knew that I wanted an occupation where I could work with my hands but also make a positive difference in people’s lives. I can think of no field in medicine that is more creative, gratifying, or exciting.”
The son of artist and a clergyman, Dr. Adam Tattelbaum grew up in a household where artistry and enhancing the lives of others took equal place. “I always knew that I wanted an occupation where I could work with my hands but also make a positive difference in people’s lives. I can think of no field in medicine that is more creative, gratifying, or exciting.”
Born in New York City, Dr. Tattelbaum has performed plastic surgery in the Metropolitan Washington D.C. area for almost 30 years. Trained at Columbia, Harvard and Georgetown University, Dr. Tattelbaum is certified by both the American Board of Plastic Surgery and the American Board of Surgery. He is a member of the American Society of Plastic Surgeons as well as the American Society of Aesthetic Plastic Surgery which serves as a mark of distinction in cosmetic plastic surgery. He serves on the clinical faculty at Georgetown University, where he has taught. Listed on multiple occasions as a Washingtonian and Bethesda Magazine Top Doctor, his greatest joy is the teaching and education of his patients. He offers a common sense approach to cosmetic surgery and offers the same advice to patients that he would offer to his family and friends.
Husband and proud father of two, Dr. Tattelbaum and his wife live in Maryland.
